Menopause as a Fascial Event
“The body speaks from beneath the skin.”
Menopause as a Fascial Event
Today, I listened to a client describe a frustrating experience, one of many along the path toward hip surgery. She had been moving through consultations, evaluations, and decisions about pain management, and found herself sitting across from a physician, trying to explain something that, to her, had become essential. She spoke about her fascia, about her work with another doctor who was considering postmenopausal bio-neurological changes as part of her treatment plan, and about her decision to pursue hyaluronic acid injections instead of cortisol, not simply for pain relief, but because of how her body was responding at a deeper level. Part of her management plan now included an awareness of the changes in her fascial system and the ways those changes were expressing themselves not only as pain, but through her skin. She described extreme dryness, chronic itching without any visible rash, and a level of irritation that moved across her body without clear cause. In her conversations with a more informed physician, she had begun to understand that with the postmenopausal loss of hormones, particularly estrogen, there is a measurable decrease in cellular hydration, that the tissues lose fluid, the skin barrier becomes more fragile, and the connective matrix beneath the skin, the fascia, becomes less supple, less able to glide, less able to hold moisture. What begins internally can surface as what is often dismissed as menopausal itch.
She was trying to bring this understanding into the room, and as she spoke, she could feel the disconnect. She knew she was speaking a language he did not recognize. What had become clear and embodied in her own experience sounded, to him, abstract, unfamiliar, even questionable. He challenged her, asked where her information was coming from, and what she was left with, more than anything, was not disagreement, but the quiet frustration of knowing something in her own body that had not yet been named or fully understood in the systems meant to support her. As she spoke, something in me shifted, because what she was describing was not foreign to me. For months now, I have been living inside a different expression of that same pattern. I have been itching, scratching, living with a level of skin irritation that is difficult to explain and even harder to resolve. There is no rash, no clear diagnosis, no obvious pathology, only a constant, low-grade, sometimes overwhelming sensation that something is not right, a growing discomfort, a subtle but persistent sense of disconnection from my own skin. And as I listened to her describe the relationship between hormonal change, fascial dehydration, and the way the body begins to signal through sensation, something began to link, not as an idea, but as a recognition in my own body. Because the experience she was naming in one part of the body, through pain and connective tissue, was not separate from what I had been feeling across the surface of my own.
There is something quietly annoying about the fact that science are only now beginning to name what millions of us have been living through for decades.
Millions of postmenopausal women are living in bodies that feel dry, itchy, and increasingly unfamiliar, and most of us have had no clear understanding of what is happening or how to respond to it. We wake in the night scratching our arms or legs without any visible rash, feel a persistent irritation beneath our clothing that no fabric seems to soothe, notice our skin becoming thin, papery, and overly sensitive to touch, or experience a faint crawling or prickling sensation that appears without warning and lingers without explanation.
We are told to moisturize more, to drink more water, to accept that this is simply part of aging. We try the creams, the oils, the routines that promise relief, and for a brief moment something softens, only to return again, often more insistently. What begins as dryness becomes something more complex, more intrusive, and far more difficult to name. And what stays with us is not only the discomfort, but the quiet sense that something deeper is being missed.
For years, the language offered to us has hovered around description without true understanding. “Menopausal itch.” “Hormonal pruritus.” “Neuropathic irritation.” These phrases circle the experience, but they do not hold it. They name what is happening on the surface, but not what we are actually living in our bodies. And so much of this has been carried quietly, not because we lack awareness, but because the systems meant to study and respond have not fully turned toward us.
And yet, the lives we are living tell a very different story.
We are living longer, fuller, more physically engaged lives. At seventy, we are hiking, swimming, riding horses, maintaining our yoga practice, dancing, sustaining intimacy, maintaining strength, remaining in relationship with sexual and sensual pleasure, vitality, and the world. Our bodies have not withdrawn, they are very much here, still expressive, still capable. But the models of care, the science of aging health, the importance of women’s longevity surrounding us have not kept pace with this reality.
This is where the tension becomes visible.
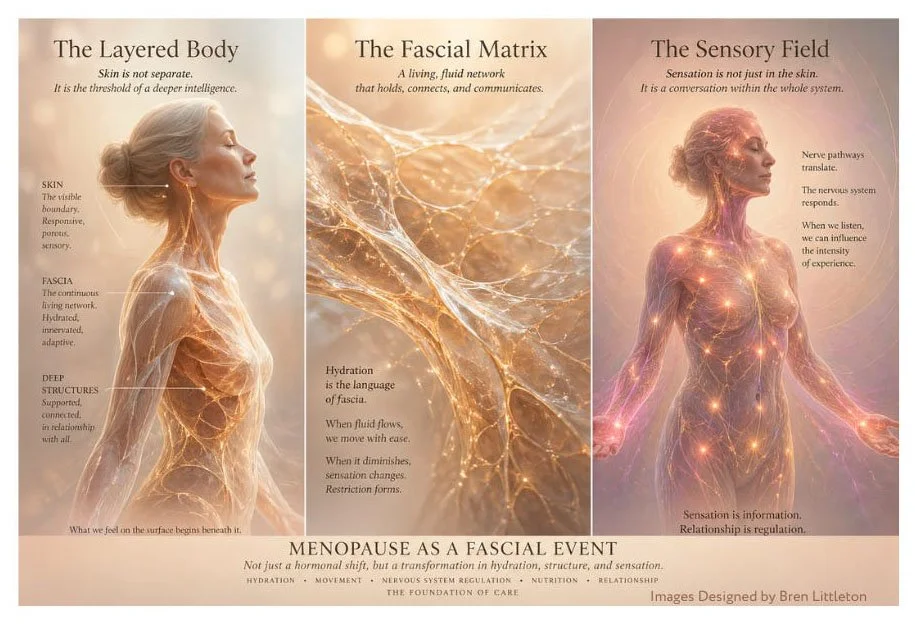
We have learned how to intervene in so many aspects of the body. We can reshape features, restore vision, replace joints, extend lifespan. And yet the largest organ of the body, our skin, along with the fascial system beneath it, remains underexamined in the context of menopause. If we begin to consider menopause not only as a hormonal event but as a fascial event, the question shifts: why is it that we can alter the structure of our faces, but not fully understand or support the changing structure of our skin and the connective tissue that gives it life?
Part of what has been missed lies just beneath the surface.
We have been trained to think of skin as something external, something to be treated from the outside. But our bodies do not organize themselves in layers of separation. Fascia, the continuous connective tissue network beneath the skin, surrounds muscles, nerves, and organs. It is living tissue, highly sensitive, richly innervated, and deeply responsive to hydration, movement, and hormonal signaling. As Robert Schleip notes in his research, fascia contains “a rich supply of sensory receptors,” suggesting that what we feel in our bodies is shaped as much by this inner network as by the skin itself. Carla Stecco’s anatomical work similarly describes fascia as a continuous, integrated system, one that does not isolate sensation but distributes it across regions of the body.
When our fascia changes, we feel different, even when the surface appears unchanged.
So when we describe itching without a rash, sensitivity without a clear cause, or a strange combination of fragility and tension, we are often describing something that involves not only the skin, but the system beneath it. This is why the prevailing explanation of dryness does not fully land. It does not account for the depth, the persistence, or the complexity of what we are feeling.
From a clinical standpoint, part of this picture is well understood. With the decline of estrogen, our bodies enter a different physiological state. Estrogen supports collagen production, lipid balance, and the presence of hyaluronic acid, all of which contribute to hydration, elasticity, and resilience. As these levels decrease, our skin becomes thinner, less able to retain moisture, and more prone to irritation.
But even here, something essential is left out.
These same changes are occurring within the fascial system. Collagen loss and reduced hydration alter the internal environment of connective tissue. The fluid matrix that allows tissues to glide becomes more dense, less responsive. Thomas Myers describes this ground substance as ideally having a “gel-like” quality that supports ease of movement between layers; when hydration diminishes, that ease is replaced by restriction, and sensation can shift along with it. We can begin to feel tighter, less at ease within ourselves. Not always visible, but deeply felt.
At the same time, our nervous systems are recalibrating. Estrogen plays a role in regulating sensory processing, including the perception of itch. As this modulation shifts, sensory nerves can become more reactive. The threshold for discomfort lowers. Sensations arise without clear dermatological cause, and they persist in ways that feel disproportionate and confusing. The work of Jean-Claude Guimberteau, who filmed living fascia in motion, reveals a dynamic, fluid architecture in constant communication, suggesting that changes in this internal environment can directly influence how sensation is generated and experienced.
Clinically, this is often labeled simply as pruritus. But even that word feels too small for what we are experiencing.
If we step back and look more honestly, what emerges is not a single condition, but a multi-system transition. Hormonal shifts. Structural changes in collagen and hydration. Skin barrier alterations. Increased sensory reactivity. And, very likely, a form of fascial dehydration that changes how we move and feel from within. To name menopause as a fascial event is to begin to see how these layers are not separate, but deeply intertwined.
These are not separate experiences. They are happening together, inside us.
And yet the research that does exist remains fragmented. Each piece is studied in isolation. Hormones in one field. Skin in another. Nervous system elsewhere. Fascia still emerging. But our bodies do not experience themselves in parts. We experience ourselves as a whole.
This is why so many of us have felt unseen within the current explanations.
It is not that nothing is known. It is that what is known has not yet been brought together in a way that reflects our lived reality.
We are, perhaps, just beginning to arrive at a more coherent understanding. Not a formal diagnosis, but a recognition of pattern. A post-estrogen shift in the neurofascial system, where skin, connective tissue, and sensory processing are all involved in a single lived experience.
To name it in this way is not to pathologize our bodies, but to respect their coherence.
Because the truth is, our bodies are not failing.
They are adapting.
They are reorganizing in response to profound internal changes, and in doing so, they are asking for a different kind of care. Not only surface treatment, but attention to hydration within the tissues, to movement that restores glide between layers, to nervous system regulation that softens sensory reactivity, to internal nourishment that supports repair and resilience.
Gentle, sustained stretching. Myofascial release through hands or simple tools. Walking, spiraling movement, anything that restores fluidity between layers. Breathwork with a longer exhale. Warm, rhythmic touch. Slow, safe awareness of the body. Adequate hydration supported by electrolytes. Omega-3 fatty acids. Nutrients that support collagen, including vitamin C and amino acids.
None of these are quick solutions. But together, they begin to form a more complete response to what our bodies are asking for when we understand menopause as a fascial event rather than a surface condition.
And still, the deeper question remains.
Why are we only now naming this?
Why has it taken so long for science to fully turn toward women’s midlife bodies, not as a niche concern, but as a central field of study? When will the same level of curiosity, funding, and integration be applied here?
Because we are not withdrawing from life.
We are still here. Still living. Still creating. Still moving in and through the world with strength, intelligence, and desire for engagement.
The naming of this experience matters.
It is not a small correction. It is the beginning of a larger shift, one that recognizes that our bodies are not problems to be managed quietly, but systems to be understood, supported, and met with the full attention they have always deserved.
What Is Beginning to Emerge
There are, quietly, other approaches beginning to enter the conversation. Not as solutions in the conventional sense, but as ways of working with the body that acknowledge the role of the nervous system, perception, and internal communication in how sensation is experienced.
Some women have found relief not by eliminating the sensation of itch, but by changing their relationship to it.
One of these approaches includes tapping, or Emotional Freedom Technique (EFT), a practice that combines light rhythmic tapping on specific points of the body with focused attention. While it does not directly alter the structure of the skin or fascia, it appears to influence how the nervous system processes sensation, lowering reactivity and softening the intensity of experience. When the threshold for discomfort is reduced, what once felt overwhelming can become more tolerable, sometimes even intermittent.
This matters more than it might first appear.
Because part of what we are encountering is not only structural, but sensory. The body is not simply dry; it is, at times, over-signaling.
And when signaling changes, our response becomes part of the experience.
There are also more inward practices that invite a different kind of engagement altogether.
In my work, I have long taught the use of Active Imagination, a Jungian method of entering into dialogue with the psyche through image, sensation, and felt experience. Traditionally, this has been used to work with anxiety, panic, pain, and emotional conflict. But the same approach can be extended to the body itself.
To the skin.
To the areas that itch, that irritate, that feel unfamiliar.
Rather than attempting to suppress or ignore the sensation, the invitation is to turn toward it, gently, and ask:
What are you trying to communicate?
What do you need?
What has changed?
This is not metaphorical work.
The body responds when it is met with attention that is neither invasive nor dismissive. Sensation, when listened to rather than resisted, often begins to shift in quality. Not always disappearing, but becoming more defined, more specific, sometimes less diffuse.
A relationship begins to form.
And within that relationship, something subtle but important changes. The body is no longer something happening to us, but something we are in communication with.
These approaches do not replace the need for medical understanding or physiological support. They do not rehydrate tissue or restore collagen directly. But they address another layer of the experience, one that is increasingly recognized as inseparable from the physical: the way the nervous system interprets and responds to what the body is signaling.
If menopause is, in part, a fascial event, then it is also a sensory one.
And perhaps part of what is on the horizon is not only better treatments, but a more integrated way of working with the body, one that includes structure, chemistry, and communication.
Not control.
But relationship.
And I find myself thinking again of my client, sitting in that room, trying to describe what she already knew in her body, trying to translate an experience that had not yet been fully recognized. The frustration she carried was not simply about being questioned, but about standing at the edge of something real without a shared language to hold it. Perhaps this is where we are now, not at the beginning of the experience, but at the beginning of its naming, learning, slowly, how to speak about what we have been living all along.
written by Bren Littleton
Tin Flea Press, c. 2026